Sildenafil in the treatment of erectile dysfunction: an overview of the clinical evidence
Erectile dysfunction (ED) is a very common condition associated not only with aging but also with risk factors such as hypertension, heart disease, obesity, dyslipidemia, diabetes, hypogonadism, medications and pelvic surgery. Many of these factors are components of metabolic syndrome, a multiple risk factor for cardiovascular disease (CVD) ED is one of the common risk factors for CVD. Endothelial dysfunction appears to be an early pathophysiology characteristic of both diseases. The efficacy, tolerability, and cardiovascular safety of sildenafil have been evaluated in a number of large randomized, double-blind, placebo-controlled clinical trials in a broad population of men with ED, including men with several comorbidities. Sildenafil is effective in some specific patient groups, including difficult-to-treat subgroups such as diabetics and individuals after radical prostatectomy. Sildenafil has a rapid onset of action (less than 14 minutes) and a duration of action of up to 12 hours in some men. Sildenafil improves quality of life and satisfaction in treated men, is well tolerated and has a good safety profile. New evidence suggests that sildenafil has favorable effects in a number of chronic diseases. Sildenafil is approved for the treatment of idiopathic pulmonary hypertension. Several studies have suggested that it improves endothelial function, as well as its possible role in the treatment of premature ejaculation and lower urinary tract symptoms.
Introduction
Erectile dysfunction (ED) is a major sexual problem for men and a very common condition. The prevalence of ED increases with age: the Massachusetts Male Aging Study (MMAS) found that the prevalence of ED in men aged 40 years is 40%, increasing to nearly 70% in men aged 70 years. The MMAS study found that the prevalence of ED in men aged 40 years increased from 40% to nearly 70% in men aged 70 years. As the proportion of older people in the population increases, the global prevalence of ED is estimated to double from 152 million in 1995 to 322 million by 2025 ED is also associated with other conditions such as aging, smoking, hypertension, heart disease, diabetes, and the effects of radical prostatectomy. Cardiovascular disease (CVD) and ED share common risk factors reflecting endothelial dysfunction. In men without prior CVD, ED is the first sign of CVD and may develop well before CVD, with a median duration of 3 years. With the advent of phosphodiesterase type 5 inhibitors (PDE5i), the number of patients with erectile function problems has increased, but the medical treatment of ED has also undergone significant changes. More physicians are prescribing PDE5i, which has proven efficacy and safety, to treat ED with minimal evaluation, especially in primary care. Treatment of ED by non-specialist physicians, mainly due to lack of time and knowledge, minimizes patient evaluation and prescribes only first-line drugs. Sildenafil is the first PDE5i to revolutionize the treatment of ED: as of July 2006, more than 2,600 articles have been published in Medline, and extensive experience and research has led to more than 30 million men worldwide being treated with sildenafil. In addition, new evidence suggests that sildenafil has favorable effects in a number of chronic diseases. Recently approved for the treatment of idiopathic pulmonary hypertension, PDE5i may improve endothelial function; it is also hypothesized that PDE5i may be beneficial for patients with premature ejaculation. However, it is still unclear in clinical studies whether PDE5i acts on the physiological process of ejaculation or indirectly improves erectile function and thus reduces performance anxiety in men with ED. The aim of this review is to provide an overview of the clinical data regarding the use of sildenafil for the treatment of ED, as well as data from ongoing basic and clinical studies in other chronic diseases.
Pharmacological profile: time of onset of action and duration of action
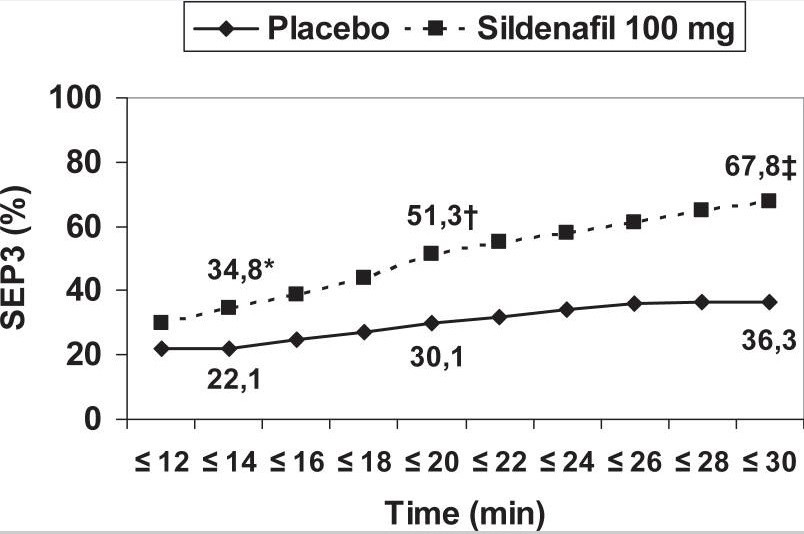
Cenforce Sildenafil is a highly selective type 5 PDE inhibitor. Sildenafil enhances NO-mediated relaxation of the human corpus cavernosum in vitro. Sildenafil increases intracellular concentrations of cyclic guanosine-3′,5′ monophosphate (cGMP) by inhibiting phosphodiesterase, resulting in enhancement of the endogenous NO-cGMP signaling pathway. The time to reach maximum plasma concentration is about 1 hour and the plasma elimination half-life is about 4-5 hours. 25 mg, 50 mg and 100 mg are administered orally as needed. The recommended starting dose is 50 mg and may be increased or decreased as needed depending on efficacy and tolerability. Patients should be instructed to take sildenafil approximately 1 hour before sexual intercourse, with a maximum dose of once daily. Sexual stimulation is a prerequisite for sildenafil administration as for other PDE5i. The possibility of sexual intercourse persists from 30 minutes to 4-5 hours after taking the drug. However, onset of action occurs after 14 minutes in about 35% of patients (Figure (Figure 1)1) (Padma-Nathan et al 2003) and efficacy may persist for up to 12 hours (Moncada et al 2004). A high fat diet reduces absorption and increases absorption time. Alcohol does not affect absorption at usual doses.
Use of sildenafil in aging men
Normal aging processes and the accumulation of age-related risk factors contribute to the increased prevalence of erectile dysfunction in older age. Systemic changes and alterations in penile structure and function in older men include hormonal changes (mainly decreased testosterone levels and decreased bioavailability of testosterone due to increased levels of sex hormone-binding globulin), decreased elastic fibers and increased collagen fibers in the tunica media, and molecular changes (decreased levels of nitric oxide synthase). Plasma concentrations of sildenafil are higher in older men (65 years and older) than in younger men (18-45 years), with mean maximum concentration (Cmax) 70% higher in older men and mean area under the curve (AUC) 84% higher than in younger men. Due to age-related differences in binding to plasma proteins, the corresponding increase in free sildenafil plasma concentration was about 40%. However, no safety differences were observed with any dose of sildenafil compared to young men. Therefore, dose adjustment in elderly patients is not required. Sildenafil significantly improves erectile function in elderly patients with erectile dysfunction of various etiologies, but may have lower efficacy compared to young men due to the normal aging process and accumulation of age-related risk factors described above.
Conclusions
Cenforce (Sildenafil) is a highly effective drug with a good safety and tolerability profile in men with ED. Sildenafil is less effective in so-called intractable groups, such as patients with diabetes mellitus and men after radical prostatectomy, but is also effective in some groups, including elderly men. Sildenafil significantly improves satisfaction and quality of life for both patients and their partners. In addition, new data from basic and clinical studies suggest a possible future role for the drug in a number of other chronic diseases.









Comment